
Clinical Presentation:
• High BP of pregnant lady beyond 20 weeks of gestation.
• Proteinuria.
• End organ changes.
• No complaints of any headache, nausea, vomiting, abdominal pain or visual changes.
Severe preeclampsia:
• BP shooting more than 160/110 mm Hg
• Any end organ changes
Pathophysiology:
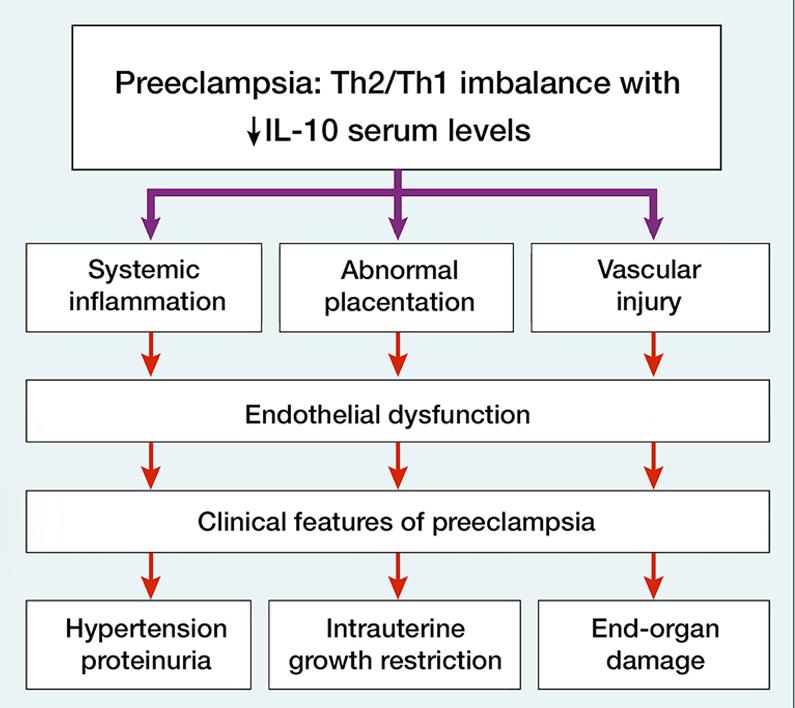
Incomplete trophoblast invasive spiral arterioles causes defective remodeling of spiral artery. Therefore, spiral arterioles remain narrow causing placental ischemia. This causes release of inflammatory mediators leading to endothelial damage.
Endothelial damage leads to:
• Vasospasm and ischaemic sequelae – blood flow to different organs get compromised.
• Leaky capillaries – fluid moves out to interstitial space from vessels causing hemoconcentration (whereas normally in pregnant women hemodilution occurs).
• Thrombotic sequelae – it causes deposition of platelets and clotting factors.
Vasospasm and ischaemic sequelae causes:
• Retinal ischemia
• Hypertension
• Hepatic necrosis
Leaky capillaries causes:
• Edema
• Cerebral edema
• Pulmonary edema
• Proteinuria
Thrombotic sequelae causes:
• Platelet count decreases
• Disseminated intravascular coagulation (DIC)
• Risk of placental abruption due to thrombosis in placental circulation (also causes intrauterine growth retardation of fetus).
Risk factors of preeclampsia:
• History of preeclampsia in previous pregnancy
• Extremes of maternal age (young and old)
• Multiple pregnancy
• Obesity
• Chronic hypertension
• Diabetes mellitus
• Chronic kidney disease
• Primipara
• Molar pregnancy
• Prolonged interpregnancy interval
• Anti phospholipid antibody syndrome
Management of preeclampsia:
• Baseline investigation and workup
• Keep a control BP
• Keep a watch on development of severe preeclampsia
• Keep a watch for fetal growth and well being
If ,
– there is mild preeclampsia
– BP is well controlled
– baby and mother are doing well
Then,
Terminate pregnancy after 37 weeks of completed intrauterine life
(Go for vaginal delivery or caesarean section)
Investigations to look for end organ changes:
• Complete blood count
• Kidney function test
• Liver function test
• Check for evidence of pulmonary edema
• Ask about epigastric and right hypochondriac pain
• Ask about any complaints of headache and blurring of vision
BP control:
Control of BP is done to prevent placental abruption, intracerebral bleeding and acute hypertensive complications.
Drugs to control BP:
• Labetalol (drug of choice)
• Methyl dopa
• Nifedipine (calcium channel blockers)
• Hydralazine
Other drugs are contraindicated because they are teratogenic causing oligohydramnios.
Diuretics are also contraindicated in this case.
Management of severe preeclampsia:
1. Admit the woman
2. Perform baseline investigations and follow-up
3. Control BP and keep on monitoring it
4. Watch for sign and symptoms for impeding eclampsia
5. USG and fetal Doppler – to evaluate well being of baby
6. Give steroids for maturation of lungs of fetus if baby is <34 weeks of gestational age and continue monitoring baby and mother.
7. If baby is >34 weeks of gestational age and signs of severe preeclampsia seen, termination of pregnancy.
8. Baby <34 weeks of IUL, and signs and symptoms of impeding eclampsia seen with uncontrolled BP, pulmonary edema, placental abruption, fetal distress, eclampsia, liver dysfunction, kidney dysfunction, HELLP syndrome (hemolysis, elevated liver enzymes, low platelets) then termination of pregnancy is done irrespective of period of gestation.
None of the drug listed above should be taken without proper consultation of the doctor.This post is just for educational purpose and not for any clinical purpose.
Contributor- Medico Eshika Keshari
Knowledgeable