-a normal menstrual cycle is usually of 28 days measured by the time between the first day of one period and first day of next.
-duration of bleeding is 4-6 days and estimated blood loss is around 80ml.
-the deviation of ±7 days from 28 days rhythm is common.
-menstrual rhythm depends on hypothalamic pituitary axis function and amount of blood loss depends upon uterine condition.
Definitions of menstrual cycle irregularities:
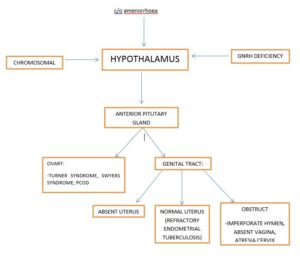
1. Amenorrhoea: absence of menstruation.
• it is a symptom, not a disease.
• Physiological amenorrhoea: naturally prevails prior to onset of puberty, during pregnancy and lactation and after menopause.
• Pathological amenorrhoea: result from genetic factors, systemic disease, endocrinopathies, and disturbance in hpo axis, gynatresia, environmental factors, drugs usage, and psychological factors.
• Primary amenorrhoea: failure of onset of menstruation beyond age of 16years regardless of development of secondary sexual characters.
• Secondary amenorrhoea: failure of occurance of menstruation for 6 months longer in a female who have previously menstruated.
• Diagnosis presenting clinically as primary amenorrhoea can be classified according to the status of serum FSH levels.
-hypergonadotropic primary amenorrhoea
-eugonadotropic primary amenorrhoea
-hypogonadotropic primary amenorrhoea
2. Oligomenorrhoea: the cycle length exceeds 35 days without any impairment of fertility.
-amenorrhoea is often continnum of oligomenorrhoea.
-this condition is often encountered in females at extremes of reproductive life and in some lactating females.
3. Hypomenorrhoea:
– in some females, menstruation lasts for only 1-2 days and blood loss is too scanty.
-scanty, otherwise normal menstruation may not be pathological since its regularity presupposes a normal hypothalmic-pitutary-ovarian relation.
-in these females, uterine end organ may be at fault.
4. Polymenorrohea:
-also known as epimenorrhoea
-frequent episodes of menstruation at interval of 21 day or less.
-shortened cycles
-menorrhagia goes hand in hand with this.
-more frequent in adolescent females and perimenopausal females.
-exact cause of problem is basically unknown.
-in most females the follicular phase is accelerated leading to shorter cycles.
-polymenorrhagia is frequently observed when female resumes menstrual activity after delivery, attributed to persistence activity of anterior lobe of pitutary gland, initiated during pregnancy into post natal phase.The excess stimulation from gonadotropin causes frequent ovulation and menstruation.
5. Metrorrhagia:
– intermenstrual bleeding.
-acyclic bleeding from genital tract and not restricted to uterus only.
-it may be intermittent/continuous and superimposed on normal menstrual cycle.
– it can be physiological occuring at the time of ovulation, this mid menstrual bleed lasts for few hours to one day with a profuse sticky discharge and intermittent cramp pain.
– in elderly females post-coital bleeding not to be ignored as it may be earliest sign of neoplasm.
6. Menometrorrhagia: excessive, prolonged, bleeding that occurs at irregularly timed and frequent intervals.
7. Menorrhagia: regularly timed episodes of bleeding that are excessive in amount (>80ml) and/or duration of flow >5days.
8. Precocious menstruation: occurance of menstruation before 10 years of age.
9. Post-coital bleed: vaginal bleeding after sexual intercourse.
•The causes of various menstrual cycle disorders are different and the diagnosis depends on the clinical and lab investigations, similarly the treatment protocols are different based on the diagnosis.
Contributor- Dr. Yagika pareek
👏👏
Informative👏👏👏👏
Very informative and we’ll explained